

Potpourri...
Well hello everyone! Long time no see. I thought maybe I'd make a post so that people know I'm still alive and doin' my thing. I got a few emails concerned that I had given up and I want everyone to know that that is not the case. In fact just the opposite. I've been trying to really kick it into gear. The problem I've been having is still the sleep and it's just been hard to concentrate and I haven't felt like posting much.
Let's recap what's been going on since we last spoke...Well it's pretty much the same. I'm still working on trying to get my sleeping habits back to normal. I'm waiting to speak with a specialist about sleep disorders. In the mean time I'm going to have to tell my Dr that the last RX he gave me is just not regulating my sleep and I'm still getting 2 or so hours a night and then crashing for a day every 3 or 4 days.
On the good side I did start water cardio with my trainer and have tried a couple of times on my own and I like it quite a bit. We've decided to make our saturday workout a water day and I've tried to get into the pool at least 1 or 2 times a week outside of that.
Also, I'm going to measure and weigh in at the end of next week, for those of you who keep up on that with me. Probably Thursday or Friday depending when I can get all the numbers together for you...that should be fun ;0)
That's about it.
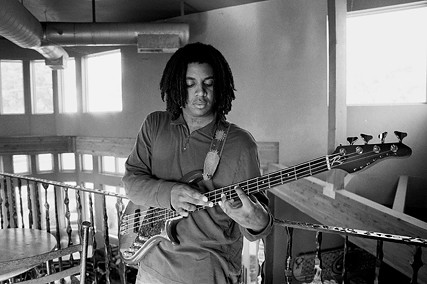
In other news. A long time ago I was really into Photography. Did it for a living for a while but got a little burned out. (I know...I know..."how many hobbies does this guy have...writing lame stories, making puppets, photography?") anyhoo, I used to have a really nice camera which for financial reasons I had to pawn a long while back...Don't worry it's not all that bad...I kept up with paying the interest on the loan and just the other day I was finally able to pay off the original loan and I got my camera back! For those of you 'in the know', it's a Canon 1v...the last pro 35mm film camera they made but it's super sweet and kicks alllll sorts of hind end! Wha-hoo! *Doin' a dance....shak'ah shak'ah!!* This whole blog thing has really got my creative juices flowing and I want to create...I still plan to do the podcast as soon as I start to show a steady loss (so I have something to talk about) and I still plan to get my next puppet started sometime soon and now that I have my camera back I want to start photographing local bands again. I dug up a few samples of my work for you to look at. You're welcome to let me know what you think.

Bob's Child
Brian Rogers

ALTA
I also thought I'd show you a short clip of my friend Justin Farren playing at a show I went to last weekend. Great show and great folks...I can't wait for the next one!
That's it for now...I'm drowsey but somehow wired at the same time. I'm gonna try to close my eyes and see if anything comes of it. I just hope that closet stays closed until I'm really asleep this time. I do not want to go through that again...'shivers'...
Let's recap what's been going on since we last spoke...Well it's pretty much the same. I'm still working on trying to get my sleeping habits back to normal. I'm waiting to speak with a specialist about sleep disorders. In the mean time I'm going to have to tell my Dr that the last RX he gave me is just not regulating my sleep and I'm still getting 2 or so hours a night and then crashing for a day every 3 or 4 days.
On the good side I did start water cardio with my trainer and have tried a couple of times on my own and I like it quite a bit. We've decided to make our saturday workout a water day and I've tried to get into the pool at least 1 or 2 times a week outside of that.
Also, I'm going to measure and weigh in at the end of next week, for those of you who keep up on that with me. Probably Thursday or Friday depending when I can get all the numbers together for you...that should be fun ;0)
That's about it.
In other news. A long time ago I was really into Photography. Did it for a living for a while but got a little burned out. (I know...I know..."how many hobbies does this guy have...writing lame stories, making puppets, photography?") anyhoo, I used to have a really nice camera which for financial reasons I had to pawn a long while back...Don't worry it's not all that bad...I kept up with paying the interest on the loan and just the other day I was finally able to pay off the original loan and I got my camera back! For those of you 'in the know', it's a Canon 1v...the last pro 35mm film camera they made but it's super sweet and kicks alllll sorts of hind end! Wha-hoo! *Doin' a dance....shak'ah shak'ah!!* This whole blog thing has really got my creative juices flowing and I want to create...I still plan to do the podcast as soon as I start to show a steady loss (so I have something to talk about) and I still plan to get my next puppet started sometime soon and now that I have my camera back I want to start photographing local bands again. I dug up a few samples of my work for you to look at. You're welcome to let me know what you think.
I also thought I'd show you a short clip of my friend Justin Farren playing at a show I went to last weekend. Great show and great folks...I can't wait for the next one!
That's it for now...I'm drowsey but somehow wired at the same time. I'm gonna try to close my eyes and see if anything comes of it. I just hope that closet stays closed until I'm really asleep this time. I do not want to go through that again...'shivers'...
posted by Sean Perkey at Friday, September 29, 2006
6 comments
![]()
![]()












